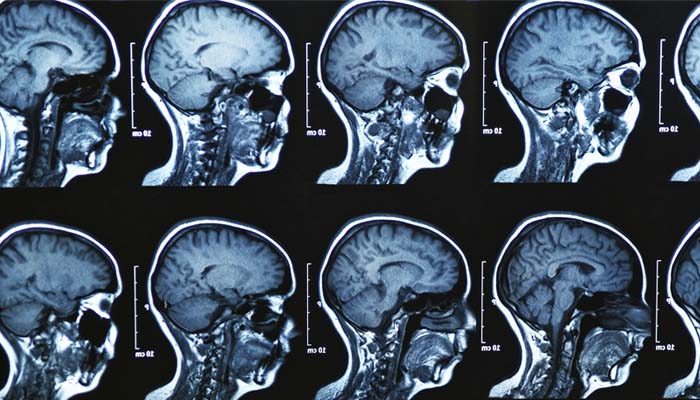
The brains of humans and other vertebrates are composed of very soft tissue and have a gelatin-like texture. Living brain tissue has a pink tint in color on the outside (gray matter), and nearly complete white on the inside (white matter), with subtle variations in color. The three largest divisions of the brain are:
Cerebral cortex
Brainstem
Cerebellum
These areas are composed of two broad classes of cells: neurons and glia. These two types are equally numerous in the brain as a whole, although glial cells outnumber neurons roughly 4 to 1 in the cerebral cortex. Glia come in several types, which perform a number of critical functions, including structural support, metabolic support, insulation, and guidance of development. Primary tumors of the glial cells are called gliomas and often are malignant by the time they are diagnosed.
What is Brain Tumor?
A brain tumor occurs when abnormal cells form within the brain. There are two main types of tumors: malignant tumors and benign (non-cancerous) tumors. These can be further classified as primary tumors, which start within the brain, and secondary tumors, which most commonly have spread from tumors located outside the brain, known as brain metastasis tumors. All types of brain tumors may produce symptoms that vary depending on the size of the tumor and the part of the brain that is involved. Where symptoms exist, they may include headaches, seizures, problems with vision, vomiting and mental changes.Other symptoms may include difficulty walking, speaking, with sensations, or unconsciousness.
The most common primary brain tumors are:
Gliomas :
A glioma is a type of tumor that starts in the glial cells of the brain or the spine. Gliomas comprise about 30 percent of all brain tumors and central nervous system tumours, and 80 percent of all malignant brain tumours.High-grade gliomas are highly vascular tumors and have a tendency to infiltrate diffusely. They have extensive areas of necrosis and hypoxia. Often, tumor growth causes a breakdown of the blood–brain barrier in the vicinity of the tumor. As a rule, high-grade gliomas almost always grow back even after complete surgical excision, so are commonly called recurrent cancer of the brain.Gliomas are classified by cell type, by grade, and by location.
Treatment for brain gliomas depends on the location, the cell type, and the grade of malignancy. Often, treatment is a combined approach, using surgery, radiation therapy, and chemotherapy. A prolonged survival was observed when treating with radiotherapy and concomitant temozolomide. Radiotherapy was given for 5 days a week for 6 week, with a total of 60 Gy. Temozolomide was given daily during the treatment of radiotherapy, at a dose of 75 mg per square meter of body surface area per day. When radiotherapy ended additionally six cycles of temozolomide were given, for five days during each cycle of 28 days.
The neoplasms currently referred to as meningiomata were referred to with a wide range of names in older medical literature, depending on the source. Various descriptors included “fungoid tumors”, “fungus of the dura mater”, “epithelioma”, “psammoma”, “dural sarcoma”, “dural endothelioma”, “fibrosarcoma”, “angioendothelioma”, “arachnoidal fibroboastoma”, “endotheliosis of the meninges”, “meningeal fibroblastoma”, “meningoblastoma”, “mestothelioma of the meninges”, “sarcoma of the dura”, and others
Meningiomata usually can be surgically resected (removed) and result in a permanent cure if the tumor is superficial on the dural surface and easily accessible. Transarterial embolization has become a standard preoperative procedure in the preoperative management. If invasion of the adjacent bone occurs, total removal is nearly impossible. It is rare for benign meningiomata to become malignant.
Meningiomas :
Meningioma, also known as meningeal tumor, is typically a slow-growing tumor that forms from the meninges, the membranous layers surrounding the brain and spinal cord. Symptoms depend on the location and occur as a result of the tumor pressing on nearby tissue. Many cases never produce symptoms. Occasionally seizures, dementia, trouble talking, vision problems, one sided weakness, or loss of bladder control may occur.
Meningiomata arise from arachnoidal cap cells, most of which are near the vicinity of the venous sinuses, and this is the site of greatest prevalence for meningioma formation. Some subtypes may arise from the pial cap cells that migrate during the development together with blood vessels into the brain parenchyma.
Pituitary adenomas:
The pituitary gland or hypophysis is often referred to as the “master gland” of the human body. Part of the hypothalamic-pituitary axis, it controls most of the body’s endocrine functions via the secretion of various hormones into the circulatory system. The pituitary gland is located below the brain in a depression (fossa) of the sphenoid bone known as the sella turcica.
Pituitary adenomas are tumors that occur in the pituitary gland. Pituitary adenomas are generally divided into three categories dependent upon their biological functioning: benign adenoma, invasive adenoma, and carcinomas.Treatment options depend on the type of tumor and on its size.Pituitary incidentalomas are pituitary tumors that are characterized as an incidental finding. They are often discovered by computed tomography (CT) or magnetic resonance imaging (MRI), performed in the evaluation of unrelated medical conditions such as suspected head trauma, in cancer staging or in the evaluation of nonspecific symptoms such as dizziness and headache.
Nerve sheath tumors :
A nerve sheath tumor is a type of tumor of the nervous system (nervous system neoplasm) which is made up primarily of the myelin surrounding nerves.A peripheral nerve sheath tumor (PNST) is a nerve sheath tumor in the peripheral nervous system. Benign peripheral nerve sheath tumors include schwannomas and neurofibromas.A malignant peripheral nerve sheath tumor (MPNST) is a cancerous peripheral nerve sheath tumor.
Brief introduction of other brain tumors :
Glioblastomas (GBMs):
are one of the most devastating primary tumors in humans and often results in minimal survival rates.Glioblastoma multiforme (GBM) is one of the most aggressive primary tumors in adults. Despite vigorous efforts and novel treatment approaches to reduce their impact on mortality, the median overall survival rate remains approximately 12–16 months.
Astrocytoma :
Astrocytomas are a type of brain tumor. They originate in a particular kind of glial cells, star-shaped brain cells in the cerebrum called astrocytes. This type of tumor does not usually spread outside the brain and spinal cord and it does not usually affect other organs.Astrocytoma causes regional effects by compression, invasion, and destruction of brain parenchyma, arterial and venous hypoxia, competition for nutrients, release of metabolic end products (e.g., free radicals, altered electrolytes, neurotransmitters), and release and recruitment of cellular mediators (e.g., cytokines) that disrupt normal parenchymal function.
There are no precise guidelines because the exact cause of astrocytoma is not known.For low-grade astrocytomas, removal of the tumor generally allows functional survival for many years. In some reports, the 5-year survival has been over 90% with well-resected tumors. Indeed, broad intervention of low-grade conditions is a contested matter. In particular, pilocytic astrocytomas are commonly indolent bodies that may permit normal neurologic function. However, left unattended, these tumors may eventually undergo neoplastic transformation.
Craniopharyngioma :
A craniopharyngioma is a rare type of brain tumor derived from pituitary gland embryonic tissue that occurs most commonly in children, but also affects adults. It may present at any age, even in the prenatal and neonatal periods, but peak incidence rates are childhood-onset at 5–14 years and adult-onset at 50–74 years.Craniopharyngioma is a rare, usually suprasellar neoplasm, which may be cystic, that develops from nests of epithelium derived from Rathke’s pouch. Rathke’s pouch is an embryonic precursor of the anterior pituitary.
Craniopharyngiomas are almost always benign. However, as with many brain tumors, their treatment can be difficult, and significant morbidities are associated with both the tumor and treatment. Headache (obstructive hydrocephalus),
Hypersomnia,MyxedemaPostsurgical weight gain,Polydipsia,Polyuria (diabetes insipidus) ,Vision loss (bitemporal hemianopia).
Treatment generally consists of subfrontal or transsphenoidal excision. Endoscopic surgery through the noseoften performed by a joint team of neurosurgeons and ENT, is increasingly being considered as an alternative to transcranial surgery done by making an opening in the skull.Current research has shown ways of treating the tumors in a less invasive way while others have shown how the hypothalamus can be stimulated along with the tumor to prevent the child and adult with the tumor to become obese. Craniopharyngioma of childhood are commonly cystic in nature. Limited surgery minimizing hypothalamic damage may decrease the severe obesity rate at the expense of the need for radiotherapy to complete the treatment.
Brain tumors in infants
Brain tumors in infants have different clinical presentations, anatomical distribution, histopathological diagnosis, and clinical prognosis compared with older children.Brain tumors in infants should be treated with surgical resection, followed by chemotherapy when necessary.Central nervous system (CNS) tumors are among the most common neoplasms in children. Intracranial tumors with the onset of symptoms before the age of 1 year once were considered to be rare; however, increasing numbers of such tumors have been detected in recent decades thanks to widespread use of modern imaging techniques.
he histological distribution of malignant to benign brain tumors is higher in neonates (100%) and infants (53%) compared with older children (43%). According to a worldwide study by Di Rocco, the ten most common types of brain tumors in infancy are, in descending order, astrocytoma, medulloblastoma, ependymoma, choroid plexus papilloma, primitive neuroectodermal tumor (PNET), teratoma, sarcoma, meningioma, ganglioglioma, and neuroblastoma.
According to the previous investigations, the survival among patients younger than 1 year of age was less than that of older patients. Poor prognosis and high mortality in this age group have been attributed to the risks of anesthesia, difficulty in postoperative care, lack of voluntary control of water and salt intake, and the biological behavior of tumor itself

MRI :
Brain tumor patients often experience functional deficits that extend beyond the tumor site. While resting-state
functional MRI (rsfMRI) has been used to map such functional connectivity changes in brain tumor patients, the
interplay between abnormal tumor vasculature and the rsfMRI signal is still not well understood. Therefore,
there is an exigent need for new tools to elucidate how the blood‑oxygenation-level-dependent (BOLD) rsfMRI
signal is modulated in brain cancer. In this initial study, we explore the utility of a preclinical model for
quantifying brain tumor-induced changes on the rsfMRI signal and resting-state brain connectivity. We demonstrate that brain tumors induce brain-wide alterations of resting-state networks that extend to the contralateral hemisphere, accompanied by global attenuation of the rsfMRI signal. Preliminary histology suggests
that some of these alterations in brain connectivity may be attributable to tumor-related remodeling of the
neurovasculature. Moreover, this work recapitulates clinical rsfMRI findings from brain tumor patients in terms
of the effects of tumor size on the neurovascular microenvironment. Collectively, these results lay the foundation
of a preclinical platform for exploring the usefulness of rsfMRI as a potential new biomarker in patients with
brain cancer.
Magnetic Resonance Imaging (MRI) can generate mass amounts of data within a narrow time frame. Furthermore, it is safer than and not as invasive as other imaging techniques . The most popular areas for examination have been the spine and head, over the last ten years. In fact, more than half of the MRI scans have been concentrated on these areas of the body. Disorders of the central nervous system, backbone, and spine have been commonly analyzed with this technique, as well as cardiovascular system diseases and disorders of the extremities.









